5.5
Consciousness-Altering Drugs
In Jerusalem, hundreds of Hasidic men celebrate the completion of the annual reading of the holy Torah by dancing for hours in the streets. For them, dancing is not a diversion; it is a path to religious ecstasy. In South Dakota, several Lakota (Sioux) adults sit naked in the darkness and crushing heat of a sweat lodge; their goal is euphoria, the transcendence of pain, and connection with the Great Spirit of the Universe. In the Amazon jungle, a young man training to be a shaman, a religious leader, takes a whiff of hallucinogenic snuff made from the bark of the virola tree; his goal is to enter a trance and communicate with animals, spirits, and supernatural forces. And some people simply sit quietly, focused intently on the private world of their innermost thoughts, absorbed in meditation as a means of enlightenment and expanded awareness. Some common alterations of consciousness are discussed more fully in the video Altered States of Consciousness.
Watch
Altered States of Consciousness
These rituals, seemingly quite different, are all aimed at release from the confines of ordinary consciousness. Because cultures around the world have devised such practices, some writers believe they reflect a human need, one as basic as the need for food and water (Siegel, 1989). William James (1902/1936), who was fascinated by alterations in consciousness, would have agreed. After inhaling nitrous oxide (“laughing gas”), he wrote, “Our normal waking consciousness, rational consciousness as we call it, is but one special type of consciousness, whilst all about it, parted from it by the filmiest of screens, there lie potential forms of consciousness entirely different.” But it was not until the 1960s, as millions of people began to seek ways to deliberately produce altered states of consciousness, that researchers became interested in the psychology, as well as the physiology, of psychoactive drugs. The filmy screen described by James finally began to lift.
Seeking Altered States of Consciousness
Classifying Drugs
A psychoactive drug is a substance that alters perception, mood, thinking, memory, or behavior by interacting with the biochemistry of brain and body. Around the world and throughout history, the most common ones have been nicotine, alcohol, marijuana, mescaline, opium, cocaine, peyote—and, of course, caffeine. The reasons for taking psychoactive drugs have varied: to alter consciousness, as part of a religious ritual, for recreation, to decrease physical pain or discomfort, and for psychological escape.
In Western societies, a whole pharmacopeia of recreational drugs exists, and new ones, both natural and synthetic, emerge every few years. Most of these drugs can be classified as stimulants, depressants, opiates, or psychedelics, depending on their effects on the central nervous system and their impact on behavior and mood (see Review5.1). Here we describe only their physiological and psychological effects.
Stimulants speed up activity in the central nervous system. They include nicotine, caffeine, cocaine, amphetamines, methamphetamine (meth), and MDMA (Ecstasy, which also has psychedelic properties). In moderate amounts, stimulants produce feelings of excitement, confidence, and well-being or euphoria. In large amounts, they can make a person anxious, jittery, and hyperalert. In very large doses, they may cause convulsions, heart failure, and death.
Amphetamines are synthetic drugs taken in pill form, injected, smoked, or inhaled. Methamphetamine is structurally similar to amphetamine and is used in the same ways; it comes in two forms, as a powder or in a freebase (purified) form, as a crystalline solid. Cocaine is a natural drug, derived from the leaves of the coca plant. Rural workers in Bolivia and Peru chew coca leaf every day without apparent ill effects. In North America, the drug is usually inhaled, injected, or smoked in the freebase form known as crack (because of the cracking sound it makes when smoked). These methods provide more rapid access to the blood and therefore the brain, giving the drug a more immediate, powerful, and dangerous effect than when coca leaf is chewed. Amphetamines, methamphetamine, and cocaine make users feel charged up but do not actually increase energy reserves. Fatigue, irritability, and depression may occur when the effects of these drugs wear off.
Depressants slow down activity in the central nervous system. They include alcohol, tranquilizers, barbiturates, and most of the common chemicals that some people inhale to try to get high. Depressants usually make a person feel calm or drowsy, and they may reduce anxiety, guilt, tension, and inhibitions. These drugs enhance the activity of GABA, the neurotransmitter that inhibits the ability of neurons to communicate with each other. In large amounts, depressants may produce insensitivity to pain and other sensations. Like stimulants, in very large doses they can cause irregular heartbeats, convulsions, and death.
People are often surprised to learn that alcohol is a central nervous system depressant. In small amounts, alcohol has some of the effects of a stimulant because it suppresses activity in parts of the brain that normally inhibit impulsive behavior, such as loud laughter and clowning around. In the long run, however, it slows down nervous system activity. Like barbiturates and opiates, alcohol can produce anesthesia, which is why people may pass out (if they don't throw up first) when they drink excessively. Over time, alcohol damages the liver, heart, and brain. Extremely large amounts of alcohol can kill by inhibiting the nerve cells in brain areas that control breathing and heartbeat. Every so often, a news report announces the death of a college student who had large amounts of alcohol “funneled” into him as part of an initiation or drinking competition. On the other hand, moderate drinking—an occasional drink or two of wine, beer, or liquor—is associated with a variety of health benefits, including a reduced risk of heart attack and stroke, and antidiabetic effects (Brand-Miller et al., 2007; Mukamal et al., 2003; Reynolds et al., 2003).
Opiates relieve pain. They include opium, derived from the opium poppy; morphine, a derivative of opium; heroin, a derivative of morphine; synthetic drugs such as methadone; and codeine and codone-based pain relievers such as oxycodone and hydrocodone. These drugs work on some of the same brain systems as endorphins do, and some have a powerful effect on the emotions. When injected, opiates can enhance the transmission of dopamine, and so produce a rush, a sudden feeling of euphoria. They may also decrease anxiety and motivation. Opiates are highly addictive and in large amounts can cause coma and even death.
Psychedelic drugs disrupt normal thought processes, such as the perception of time and space. Sometimes they produce hallucinations, especially visual ones. Some psychedelics, such as lysergic acid diethylamide (LSD), are made in a laboratory. Others, such as mescaline (from the peyote cactus), Salvia divinorum (from an herb native to Mexico), and psilocybin (from certain species of mushrooms), are natural substances. Emotional reactions to psychedelics vary from person to person and from one time to another for any individual. A “trip” may be mildly pleasant or unpleasant, a mystical revelation or a nightmare. For decades, research on psychedelics languished because of a lack of funding, but a few clinical researchers are now exploring their potential usefulness in psychotherapy, the relief of psychological distress, the treatment of anxiety disorders, and end-of-life distress (Gasser, Kirchner, & Passie, 2015; Griffiths et al., 2008). In a pilot study in which moderate doses of psilocybin were administered to 12 patients facing death from advanced-stage cancer, the drug significantly reduced their anxiety and despair (Grob et al., 2011).
Some commonly used drugs fall outside these four classifications, combine elements of more than one category, or have uncertain effects. One is marijuana, which is smoked or, less commonly, eaten in foods such as brownies; it is the most widely used illicit drug in North America and Europe. Some researchers classify it as a psychedelic, but others feel that its chemical makeup and its psychological effects place it outside the major classifications. The main active ingredient in marijuana is tetrahydrocannabinol (THC), derived from the hemp plant, Cannabis sativa. In some respects, THC appears to be a mild stimulant, increasing heart rate and making tastes, sounds, and colors seem more intense. But users often report reactions ranging from mild euphoria to relaxation or even sleepiness.
Marijuana was once regarded as a mild and harmless sedative, but its image changed in the 1930s, when books and movies began to warn about the dire consequences of “reefer madness.”
Some researchers believe that heavy smoking of the drug (which is high in tar) may increase the risk of lung damage (Barsky et al., 1998; Zhu et al., 2000). In moderate doses, it can interfere with the transfer of information to long-term memory and impair coordination and reaction times, characteristics it shares with alcohol. In large doses, it can cause hallucinations and a sense of unreality. However, a meta-analysis found only a small impairment in memory and learning among long-term users versus nonusers, less than what typically occurs in users of alcohol and other drugs (Grant et al., 2003). And there have been zero deaths reported from the use of marijuana.
Cannabis has been used therapeutically for nearly 3,000 years and is one of the fundamental herbs of traditional Chinese medicine. Its benefits have been affirmed in contemporary medicine as well. It reduces the nausea and vomiting that often accompany chemotherapy treatment for cancer and AIDS treatments; it reduces the physical tremors, loss of appetite, and other symptoms caused by multiple sclerosis; it reduces pain; it helps reduce the frequency of seizures in some patients with epilepsy; it helps clear arteries; and it alleviates the retinal swelling caused by glaucoma (Aggarwal et al., 2009; Ben Amar, 2006; Grinspoon & Bakalar, 1993; Steffens et al., 2005).
The Physiology of Drug Effects
Psychoactive drugs produce their effects by acting on brain neurotransmitters, the chemical substances that carry messages from one nerve cell to another. A drug may increase or decrease the release of neurotransmitters at the synapse; prevent the reuptake (reabsorption) of excess neurotransmitter molecules by the cells that have released them; or interfere with the receptors that a neurotransmitter normally binds to (see Chapter4). Figure5.7 shows how one drug, cocaine, increases the amount of norepinephrine and dopamine in the synapse by blocking the reuptake of these neurotransmitters following their release. Cocaine, like other drugs, also increases the availability of serotonin (Müller & Homberg, 2015).
Figure 5.7
Cocaine's Effect on the Brain
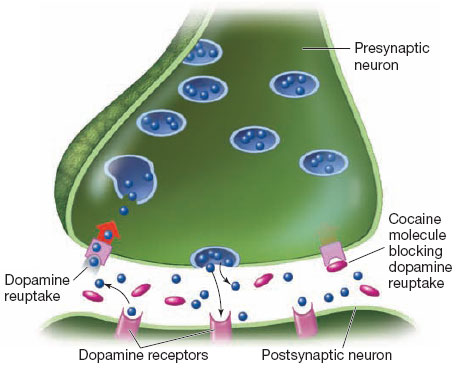
Cocaine blocks the brain's reuptake of dopamine and norepinephrine so that synaptic levels of these neurotransmitters rise. The result is overstimulation of certain brain receptors and a brief euphoric high. Then, when the drug wears off, a depletion of dopamine may cause the user to “crash” and become sleepy and depressed.
These biochemical changes affect cognitive and emotional functioning. Alcohol activates the receptor for GABA, the inhibitory neurotransmitter found in virtually all parts of the brain. Because GABA is so prevalent and modulates the activity of other neurotransmitter systems, alcohol can affect many behaviors. Just a couple of drinks can affect perception, response time, coordination, and balance, despite the drinker's own impression of unchanged or even improved performance. Alcohol also affects memory, possibly by interfering with the work of serotonin. Information stored before a drinking session remains intact during the session but is retrieved more slowly (Haut et al., 1989). Consuming small amounts does not seem to affect sober mental performance, but even occasional binge drinking—usually defined as five or more drinks on a single occasion—impairs later abstract thought. Binge-drinking college students often have impaired executive functioning: They are less able to hold on to, and work with, verbal information (Parada et al., 2012). In other words, a Saturday night binge is potentially more disabling than a daily drink.
As for other recreational drugs, there is little evidence that light or moderate use can damage the human brain enough to affect cognitive functioning, but nearly all researchers agree that heavy or frequent use is another matter. In one study, heavy users of methamphetamine had damage to dopamine cells and performed more poorly than other people on tests of memory, attention, and movement, even though they had not used the drug for at least 11 months (Volkow et al., 2001).
Under some conditions, the repeated use of some psychoactive drugs can lead to tolerance: Over time, more and more of the drug is needed to produce the same effect. When habitual heavy users stop taking a drug, they may suffer severe physical withdrawal symptoms, which, depending on the drug, may include nausea, abdominal cramps, sweating, muscle spasms, depression, disturbed sleep, and intense craving for more of the drug.
The Psychology of Drug Effects
People often assume that the effects of a drug are automatic, the inevitable result of the drug's chemistry. But reactions to a psychoactive drug involve more than the drug's chemical properties. They also depend on a person's experience with the drug, individual characteristics, environmental setting, and mental set:
Experience with the drug refers to the number of times a person has taken it. When people try a drug—a cigarette, an alcoholic drink, a stimulant—for the first time, their reactions vary markedly, from unpleasant to neutral to enjoyable. Reactions to a drug may become increasingly positive after a person has used a drug for a while and has become familiar with its effects.
The motives for using a drug, expectations about its effects, and the setting in which it is used all contribute to a person's reactions to the drug. That is why drinking alone to drown your sorrows is likely to produce a different reaction than bingeing during a competitive game of beer pong.
Individual characteristics include body weight, metabolism, initial state of emotional arousal, personality characteristics, and physical tolerance for the drug. Women generally get drunker than men on the same amount of alcohol because women are smaller, on average, so they get a higher proportionate dose of alcohol in each drink; their bodies also metabolize alcohol differently (Fuchs et al., 1995). Asians are more likely than Anglos to have a genetic variation that prevents alcohol from being metabolized normally and leads to the accumulation of a toxic substance, acetaldehyde. As a result, they tend to have adverse reactions to even small amounts of alcohol, which can cause severe headaches, facial flushing, and diarrhea (Cloninger, 1990). For individuals, a drug may have one effect after a tiring day and a different one after a rousing quarrel, or the effect may vary with the time of day because of circadian rhythms that affect various neurotransmitters. And some differences among individuals in their responses to a drug may be due to their personality traits. When people who are prone to anger and irritability wear nicotine patches, dramatic bursts of activity occur in the brain while they are working on competitive or aggressive tasks. These changes do not occur, however, in more relaxed and cheerful people (Fallon et al., 2004).
“Environmental setting” refers to the context in which a person takes the drug. A person might have one glass of wine at home alone and feel sleepy, but have three glasses of wine at a party and feel full of energy. Someone might feel happy and calm drinking with good friends, but fearful and nervous drinking with strangers. In an early study of reactions to alcohol, most of the drinkers became depressed, angry, confused, and unfriendly. Then it dawned on the researchers that anyone might become depressed, angry, confused, and unfriendly if asked to drink bourbon at 9:00 a.m. in a bleak hospital room, which was the setting for the experiment (Warren & Raynes, 1972).
“Mental set” refers to a person's expectations about the drug's effects and reasons for taking it. Some people drink to become more sociable, friendly, or seductive; some drink to try to reduce feelings of anxiety or depression; and some drink to have an excuse for abusiveness or violence. Addicts abuse drugs to escape from the real world; people living with chronic pain may use the same drugs to function in the real world. The motives for taking a drug greatly influence its effects.
Expectations can sometimes have a more powerful effect than the chemical properties of the drug itself. In several imaginative studies, researchers compared people who were drinking liquor (vodka and tonic) with those who thought they were drinking liquor but were actually getting only tonic and lime juice. (Vodka has a subtle taste, and most people could not tell the real and phony drinks apart.) The experimenters found a “think–drink” effect: Men behaved more belligerently when they thought they were drinking vodka than when they thought they were drinking plain tonic water, regardless of the actual content of the drinks. And both sexes reported feeling sexually aroused when they thought they were drinking vodka, whether or not they actually got vodka (Abrams & Wilson, 1983; Marlatt & Rohsenow, 1980).
None of this means that alcohol and other drugs are merely placebos. Psychoactive drugs, as we have seen, have physiological effects, many of them extremely potent. But by understanding the psychological factors involved in drug use, we can think more critically about the ongoing national debate over which drugs, if any, should be legal. In “Taking Psychology with You,” we discuss some points to consider as you decide what your own position is on this issue.