6.4
Other Senses
Psychological scientists have been particularly interested in vision and audition because of the importance of these senses to human survival. However, research on other senses is growing rapidly, as awareness of how they contribute to our lives increases and new ways are found to study them.
Taste: Savory Sensations
Taste, or gustation, occurs because chemicals stimulate thousands of receptors in the mouth. These receptors are located primarily on the tongue, but some are also found in the throat, inside the cheeks, and on the roof of the mouth. If you look at your tongue in a mirror, you will notice many tiny bumps; they are called papillae (from the Latin for “pimples”), and they come in several forms. In all but one of these forms, the sides of each papilla are lined with taste buds, which up close look a little like segmented oranges (see Figure6.14). Because of genetic differences, human tongues can have as few as 500 or as many as 10,000 taste buds (Miller & Reedy, 1990).
Figure6.14
Taste Receptors
The taste buds are commonly referred to, mistakenly, as the receptors for taste. The actual receptor cells are inside the buds, 15 to 50 to a bud. These cells send tiny fibers out through an opening in the bud; the receptor sites are on these fibers. New receptor cells replace old ones about every 10 days. However, after age 40 or so, the total number of taste buds (and therefore receptors) declines. Interestingly, the center of the tongue contains no taste buds. However, as in the case of the eye's blind spot, you will not usually notice the lack of sensation because the brain fills in the gap.
Four basic tastes are part of our evolutionary heritage: salty, sour, bitter, and sweet, each produced by a different type of chemical. Their receptors are tuned to molecules that alert us to good or dangerous tastes: Bitter tastes help us detect poison; sweet tastes attract us to biologically useful sugars, such as those in fruit; salty tastes enable us to identify sodium, a mineral crucial to survival; and sour tastes permit us to avoid acids in concentrations that might injure tissue (Bartoshuk & Snyder, 2012). All of the basic tastes can be perceived at any spot on the tongue that has receptors, and differences among the areas are small. When you bite into an egg or a piece of bread or an orange, its unique flavor is composed of some combination of these tastes.
Some researchers believe that we have a fifth basic taste, umami, the taste of monosodium glutamate (MSG), which is said to permit us to detect protein-rich foods; they are searching for possible receptors on the tongue for it. Umami was identified by Japanese chemists in the early 1900s as a flavor enhancer. (The word has no exact English translation, but the closest is “delicious” or “savory.”) However, findings on umami, which have largely been funded by the MSG industry, are controversial. In most foods containing protein, the umami taste is not perceptible, the way sugar is perceptible in the taste of a doughnut; and people differ widely in their responses to it (Bartoshuk, 2009).
The evidence that umami is probably not a hardwired fifth taste has led to another fascinating discovery: Taste receptors are found throughout the gastrointestinal tract and may have different functions in different locations. Protein molecules are too large to be sensed by taste or smell; but when they are eaten and digested, they are broken into their constituent amino acids, stimulating umami receptors in the gut, which in turn signal the brain that protein has been consumed, and creating a conditioned preference for the sensory properties of protein-rich foods such as bacon, roast beef, and cheese. The response to umami therefore occurs primarily in the gut, not the mouth, which would explain why a taste for protein is a learned preference rather than a universal one (Bartoshuk, 2009; Stratford & Finger, 2011).
Everyone knows that people live in what psychological scientist Linda Bartoshuk (1998) calls different “taste worlds.” Some people love broccoli and others hate it. Some people can eat burning hot chili peppers and others cannot tolerate the mildest jalapeño. And perhaps no food divides people more than cilantro. Entire websites are devoted to complaints about those innocent-looking green leaves, whose detractors think taste like soap. What causes these taste differences?
According to Bartoshuk's research, about 25 percent of people live in a “neon” taste world. These supertasters, who are overrepresented among women, Asians, Hispanics, and blacks, have an unusually large number of small, densely packed papillae (Reedy et al., 1993). For them, bitter foods such as caffeine, quinine (the bitter ingredient in tonic water), and many vegetables are unpleasantly bitter—at least twice as bitter as they are for other people. Supertasters also perceive sweet tastes as sweeter and salty tastes as saltier than other people do, and they feel more “burn” from substances such as ginger, pepper, and hot chilies (Bartoshuk et al., 1998; Lucchina et al., 1998).
Taste differences, including those between supertasters and other people, are partly a matter of genetics, but culture and learning also play a role. Many Westerners who enjoy raw food such as oysters are put off by other forms of raw seafood that are popular in Asian countries, such as sea urchin. Even within a given culture, people have different taste preferences, some of which begin in the womb or shortly after birth. Flavors as diverse as vanilla, carrot, garlic, anise, hot spices, and mint can be transmitted to the fetus or newborn through amniotic fluid or breast milk, with long-lasting consequences (Beauchamp & Mennella, 2011; Mennella et al., 2011). Babies fed salty foods prefer salty foods when they become preschoolers (Stein, Cowart, & Beauchamp, 2012).
Even illnesses can affect taste. If you have ever had an ear infection, it has probably altered the activity of a nerve that runs through your tongue and changed your perception of taste. Your experience of taste, then, is not determined by just one factor, such as genes, but also by infections, cultural preferences, exposure to other cultures' foods, and what your parents taught you. That is why you can learn to like foods that you previously thought were unappealing or “dis-tasteful.” Some former cilantro haters have learned to embrace their former herbal enemy simply by trying to like it (McGee, 2010)!
The attractiveness of a food can also be affected by its color, temperature, and texture. Even more important for taste is a food's odor. Much of what we call “flavor” is really the smell of gases released by the foods we put in our mouths. Indeed, subtle flavors such as chocolate and vanilla would have little taste if we could not smell them (see Figure6.15). Smell's influence on flavor explains why you have trouble tasting your food when you have a stuffy nose. Most people who have chronic trouble detecting tastes have a problem with smell, not taste.
Figure 6.15
Taste Test
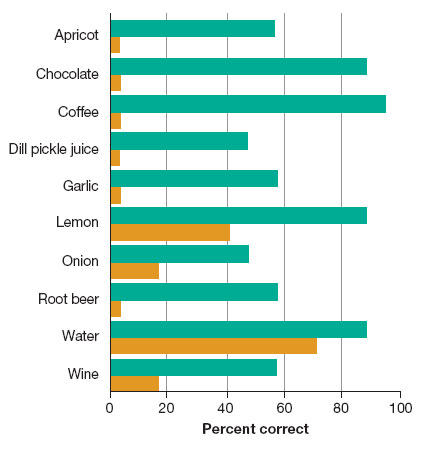
The turquoise bars show the percentages of people who could identify a substance dropped on the tongue when they were able to smell it. The orange bars show the percentage that could identify the substance when they were prevented from smelling it (Mozell et al., 1969).

Demonstrate for yourself that smell enhances the sense of taste. While holding your nose, take a bite of a slice of apple, and then do the same with a slice of raw potato. You may find that you cannot taste much difference. If you think you do taste a difference, perhaps your expectations are influencing your response. Try the same thing, but close your eyes this time and have someone else feed you the slices. Can you still tell them apart? It’s also fun to do this little test with flavored jellybeans. They are still apt to taste sweet, but you may be unable to identify the separate flavors.
Smell: The Sense of Scents
The great author and educator Helen Keller, who became blind and deaf as a toddler, once called smell “the fallen angel of the senses.” Yet our sense of smell, or olfaction, although seemingly crude when compared to a bloodhound's, is actually quite good; the human nose can detect aromas that sophisticated machines fail to detect.
The receptors for smell are specialized neurons embedded in a tiny patch of mucous membrane in the upper part of the nasal passage, just beneath the eyes (see Figure6.16). Millions of receptors in each nasal cavity respond to chemical molecules (vapors) in the air. When you inhale, you pull these molecules into the nasal cavity, but they can also enter from the mouth, wafting up the throat like smoke up a chimney. These molecules trigger responses in the receptors that combine to yield the yeasty smell of freshly baked bread or the spicy smell of a curry. Signals from the receptors are carried to the brain's olfactory bulb by the olfactory nerve, which is made up of the receptors' axons. From the olfactory bulb, they travel to a higher region of the brain.
Figure6.16
Receptors for Smell

The smell receptors’ axons make up the olfactory nerve, which carries signals to the brain. When you sniff, you draw more vapors into the nose and speed their circulation. Vapors can also reach the nasal cavity through the mouth by way of a passageway from the throat.
Figuring out the neural code for smell has been a real challenge. Of the 10,000 or so smells we detect (rotten, burned, musky, fruity, fishy, spicy . . .), none seems to be more basic than any other. Moreover, roughly 1,000 kinds of receptors exist, each kind responding to a part of an odor molecule's structure (Axel, 1995; Buck & Axel, 1991; Nakamoto, 2015). Distinct odors activate unique combinations of receptors, and signals from different types of receptors are combined in individual neurons in the brain. Some neurons seem to respond only to particular mixtures of odors rather than the individual odors in a mixture, which may explain why a mixture of clove and rose may be perceived as carnation rather than as two separate smells (Zou & Buck, 2006).
Of course, some animals have a sense of smell that makes human beings seem truly impaired by comparison. At airports, dogs detect drugs, bombs, and contraband food in people's luggage; in clinics, they detect cancer simply by sniffing a person's breath (Sonoda et al., 2011). It's not just dogs that have amazingly helpful senses of smell; in Africa, rats are helping to detect people who have undiagnosed tuberculosis (Mgode et al., 2012). The olfactory talents of many nonhuman animals evolved because smell is so important to these animals' survival.
Although smell is less vital for human survival than for the survival of other animals, it is still important. We sniff out danger by smelling smoke, rotten food, and gas leaks, so a deficit in the sense of smell is nothing to turn up your nose at. Such a loss can result from infection, disease, injury to the olfactory nerve, or smoking. A person who has smoked two packs a day for 10 years must abstain from cigarettes for 10 more years before the sense of smell returns to normal (Frye, Schwartz, & Doty, 1990).
Odors can also have psychological effects on us, which is why we buy perfumes and sniff flowers. Perhaps because olfactory centers in the brain are linked to areas that process memories and emotions, specific smells often evoke vivid, emotionally colored memories (Herz & Cupchik, 1995; Vroon, 1997). Odors can also influence people's everyday behavior, which is why shopping malls and hotels often install aroma diffusers in hopes of putting you in a good mood.
Senses of the Skin
The skin's usefulness is more than just skin deep. Besides protecting our innards, our two square yards of skin help us identify objects and establish intimacy with others. By providing a boundary between ourselves and everything else, the skin also gives us a sense of ourselves as distinct from the environment.
The basic skin senses include touch (or pressure), warmth, cold, and pain. Within these four types are variations such as itch, tickle, and painful burning. Although certain spots on the skin are especially sensitive to the four basic skin sensations, for many years, scientists had difficulty finding distinct receptors and nerve fibers for these sensations, except in the case of pressure. But then Swedish researchers discovered a nerve fiber that seems responsible for the kind of itching caused by histamines (Schmelz et al., 1997). Another team has found that the same fibers that detect pain from a punch in the nose or a burn also seem to detect the kind of pathological itch that is unrelated to histamines and that cannot be relieved by antihistamine medications (Johanek et al., 2008). Scientists have also identified a possible cold receptor (McKemy, Neuhausser, & Julius, 2002; Peier et al., 2002).
Perhaps specialized fibers will be discovered for other skin sensations as well. In the meantime, many aspects of touch remain baffling, such as why gently touching adjacent pressure spots in rapid succession produces tickle and why scratching relieves (or sometimes worsens) an itch. Decoding the messages of the skin senses will eventually tell us how we are able to distinguish sandpaper from velvet and glue from grease.
The Mystery of Pain
Pain is a sensation most of us would prefer not to experience, as shown in the video Managing Pain.
Watch
Managing Pain
Pain, which is both a skin sense and an internal sense, has come under special scrutiny. Pain differs from other senses in an important way: Even when the stimulus producing it is removed, the sensation may continue, sometimes for years. Chronic pain disrupts and can wreck a person's life, putting stress on the body and causing depression and despair. Understanding the physiology of pain has been an enormous challenge because different types of pain (from, say, a thorn, a bruise, or a hot iron) involve different chemical changes and different changes in nerve-cell activity at the site of injury or disease, as well as in the spinal cord and brain. Several chemical substances are involved and so are glial cells, the cells that support nerve cells; they release inflammatory substances that can worsen the pain (Watkins & Maier, 2003). Here, however, we focus on a general theory of pain and on the psychological factors that influence how pain is experienced.

A nurse examines Ashlyn Blocker’s feet for injuries. Because of a rare condition, Ashlyn cannot feel pain from scrapes and scratches. Severe, chronic pain causes terrible suffering for millions of people, but moderate, temporary pain is useful because it alerts us to injury.
For many years, the most influential theory of pain was the gate-control theory, which was first proposed by Canadian psychologist Ronald Melzack and British physiologist Patrick Wall (1965). According to this theory, pain impulses must get past a “gate” in the spinal cord. The gate is not an actual structure, but rather a pattern of neural activity that either blocks pain messages from the skin, muscles, and internal organs or lets those signals through. Normally, the gate is kept shut, either by impulses coming into the spinal cord from large fibers that respond to pressure and other kinds of stimulation or by signals coming down from the brain itself. But when body tissue is injured, the large fibers are damaged and smaller fibers open the gate, allowing pain messages to reach the brain unchecked. The gate-control theory correctly predicts that mild pressure, or other kinds of stimulation, can interfere with severe or protracted pain by closing the spinal gate. When we vigorously rub a banged elbow or apply ice packs, heat, or stimulating ointments to injuries, we are applying this principle.
In the gate-control theory, the brain not only responds to incoming signals from sensory nerves but is also capable of generating pain entirely on its own (Melzack, 1992, 1993). An extensive matrix (network) of neurons in the brain gives us a sense of our own bodies and body parts. When this matrix produces abnormal patterns of activity, the result is pain. The brain's ability to generate pain can help explain the many instances of severe, chronic pain that occur without any sign of injury or disease whatsoever.
Because technology now allows scientists to study pain at the molecular and cellular level, today we know that the gate-control theory, though useful, is incomplete (Mendell, 2014). Pain may also be caused by changes to the sensitivity of neurons in the central nervous system (CNS). For example, when bursts of heat are repeatedly applied to an animal's paw, pain receptors in the paw and skin are excited and remain sensitive for several hours. During that time, even a light, harmless touch will activate the pain receptors, and applying anesthetic at the site of injury will not make the pain receptors return to normal. This finding shows that changes at the CNS level can help explain how once-harmless stimuli can end up causing pain (Latremoliere & Woolf, 2009).
An extreme version of pain without injury occurs in phantom pain, in which a person continues to feel pain that seemingly comes from an arm or leg that has been amputated, or a bodily organ that has been surgically removed. Phantom limb pain afflicts up to 90 percent of amputees. The person may feel the same aching, burning, or sharp pain from sores, calf cramps, throbbing toes, or ingrown toenails that he or she endured before the surgery. Even when the spinal cord has been completely severed, amputees often continue to report phantom pain from areas below the break. Even with no nerve impulses for the spinal-cord gate to block or let through, the pain can be constant and excruciating; some sufferers commit suicide.

After his right leg was destroyed in an explosion while he was in Iraq, Army Sergeant Nicholas Paupore experienced excruciating phantom limb pain. Even morphine didn’t help. Then he underwent a simple daily procedure. A mirror was placed at a strategic angle to reflect his intact leg, tricking his brain into registering two healthy legs. The pain almost immediately subsided. A year after therapy, he had only occasional, milder pain, and needed no medication. In some patients, mirror therapy has eliminated phantom pain entirely.
A leading explanation of phantom pain is that the brain has reorganized itself: The area in the sensory cortex that formerly corresponded to the missing body part has been “invaded” by neurons from another area, often one corresponding to the face. Higher brain centers then interpret messages from those neurons as coming from the nonexistent body part (Cruz et al., 2005; Ramachandran & Blakeslee, 1998). Even though the missing limb can no longer send signals through touch and internal sensations, memories of these signals remain in the nervous system, including memories of pain, paralysis, and cramping that occurred prior to amputation. The result is an inaccurate “body map” in the brain and pain signals that cannot be shut off.
Vilayanur Ramachandran, the neurologist who first proposed this theory, has developed an extraordinarily simple but effective treatment for phantom limb pain. Ramachandran wondered whether he could devise an illusion to trick the brain of an amputee with phantom arm pain into perceiving the missing limb as moving and pain-free. He placed a mirror upright and perpendicular to the sufferer's body, such that the amputee's intact arm was reflected in the mirror. From the amputee's perspective, the result was an illusion of two functioning arms. The amputee was then instructed to move both arms in synchrony while looking into the mirror. With this technique, which has now been used with many people, the brain is fooled into thinking its owner has two healthy arms or legs, resynchronizes the signals—and phantom pain vanishes (Ramachandran & Altschuler, 2009). Neurologists have tested this method with Iraq veterans, and are finding it to be more successful than control therapies in which patients just mentally visualize having two intact limbs (Anderson-Barnes et al., 2009; Chan et al., 2007).
Most of us can experience an illusion caused by a mechanism similar to the one Ramachandran set up. Imagine that you are sitting with your arms resting on a table. Between your arms is a screen, positioned so that you can see your left arm but not your right. But in front of the screen, also in your view, rests a full-sized right arm and hand made of rubber. You are asked to focus on the rubber hand while the experimenters take two small paintbrushes and gently stroke your left hand and the rubber hand simultaneously. Do you feel the touch of the paintbrush on the rubber hand?

A demonstration of the rubber hand illusion.
Impossibly, the answer is yes! In this study of what has become known as “the rubber hand illusion,” people reported that they felt the touch of the paintbrush on the artificial hand—which, in turn, felt as though it were their own (Botvinick & Cohen, 1998; Kammers et al., 2009). These people were not delusional. Usually, our abilities to see, feel, and know what our body parts are doing are all tightly coordinated. But in the rubber hand illusion, your brain tries to reconcile the unusual situation by “adopting” the rubber arm as its own, and “disowning” your real right arm. This fascinating phenomenon has been replicated in recent studies (Barnsley et al., 2011; Longo & Haggard, 2012; Ramachandran, Krause, & Case, 2011).
The Environment Within
We usually think of our senses as pipelines to the world around us, but two senses keep us informed about the movements of our own bodies. Kinesthesis tells us where our bodily parts are located and lets us know when they move. This information is provided by pain and pressure receptors located in the muscles, joints, and tendons. Without kinesthesis, you would have trouble with any voluntary movement. Think of how hard it is to walk when your leg has “fallen asleep” or how awkward it is to chew when a dentist has numbed your jaw.
Equilibrium, or the sense of balance, gives us information about our bodies as a whole. Along with vision and touch, it lets us know whether we are standing upright or on our heads and tells us when we are falling or rotating. Equilibrium relies primarily on three semicircular canals in the inner ear (refer back to Figure6.13). These thin tubes are filled with fluid that moves and presses on hairlike receptors whenever the head rotates. The receptors initiate messages that travel through a part of the auditory nerve that is not involved in hearing.

This person obviously has exceptional kinesthetic talents and equilibrium.
Normally, kinesthesis and equilibrium work together to give us a sense of our own physical reality, something we take utterly for granted but should not. Oliver Sacks (1985) told the heart-breaking story of Christina, a young British woman who suffered irreversible damage to her kinesthetic nerve fibers because of a mysterious inflammation. At first, Christina was as floppy as a rag doll; she could not sit up, walk, or stand. Then, slowly, she learned to do these things, relying on visual cues and sheer willpower. But her movements remained unnatural; she had to grasp a fork with painful force or she would drop it. More important, despite her remaining sensitivity to light touch on the skin, she said she could no longer experience herself as physically embodied: “It's like something's been scooped right out of me,” she told Sacks, “right at the center.”
With equilibrium, we come, as it were, to the end of our senses. Every single second, millions of sensory signals reach the brain, which combines and integrates them to produce a model of reality. How does it know how to do this? Are our perceptual abilities inborn, or must we learn them? We turn next to this issue.